KEY FACTS ABOUT COW’S MILK PROTEIN ALLERGY
This website is about the management of cow’s milk protein allergy and nutritional solutions intended for infants. By continuing on this website, you accept that Nestlé supplies the information at your own request.
Are you a healthcare professional or a parent ?
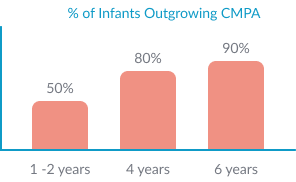
The majority of children outgrow CMPA: 50% children outgrow CMPA by 1-2 years, this increases to 80% before the age of 4. 90% of CMPA resolves by 6 years of age.1,3
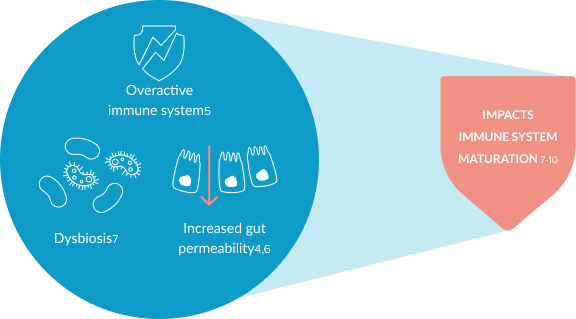
CMPA is an immune-mediated disease. It is associated with an overactive immune system, increased gut permeability and dysbiosis, which might affect the maturation of an infants’ immune system.4-10 This can lead to an increased risk of infections and future allergies.11-13